Heart disease. Lung cancer. Type II diabetes.
You. Me. The barista at the coffee shop.
For all the differences between the diseases above, each presents, if it does present, with a certain severity. For all the varied experiences of the people above, each bears some risk of developing the diseases. How do we evaluate that severity? How do measure the risk? The answer is with a score.
What is a score?
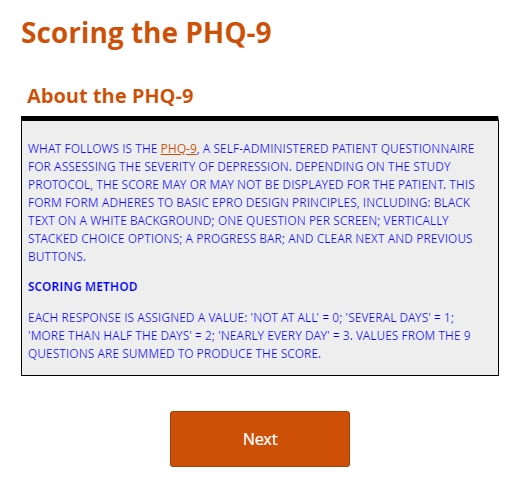
A score is a value on an ordinal scale, used to classify the severity of a condition or to predict its future course. (Only a rigorous validation study can establish if and how well the score predicts.) Instruments for generating scores take more basic measures like weight, blood pressure, or the presence or absence of some biomarker as their inputs, then combine these inputs in mathematically explicit ways. Crucially, a given score is calculated the same way from setting to setting and study to study, thus endowing the score with universal meaning.
Why are scores useful?
Scores characterize, classify, and predict. In cases of trauma or disease, a score (or a stage, or a grade) is what makes prognoses and treatment decisions possible. With scores so essential to clinical practice, it’s hardly surprising we encounter them so frequently in research. Eligibility criteria may set bounds to acceptable scores, to ensure safety or to tailor the investigation to a particular patient profile. A change in score over time may represent a primary outcome, suggesting a therapy’s superiority or inferiority to some comparator in reducing a disease burden or improving quality of life.
Scores are not comprehensive descriptions of a patient’s disease, much less of the patient herself. They are never perfectly predictive. They are quantitative heuristics whose success in classifying the stage or severity of a disease, or in predicting the risk of its development, has been established through statistical studies.
How do researchers calculate scores?
Most (not all) scores are matters of simple arithmetic. Measure A, B, and C, then add them together. If D is present, add one. If D is absent, subtract one. A researcher mentally calculating a score for one patient in a calm, quiet setting stands a good chance of doing so correctly. But as inputs grow larger (34 x 72, say, instead of 4 + 9), so does the chance of a miscalculation. Asked to perform mental calculations again and again, for dozens of study participants, the researcher is all but guaranteed to make at least one mistake.
How does EDC make working with scores easier?
When it comes to computation, it’s hard to beat, well, a computer. Collecting data electronically facilitates rapid, accurate operations on that data. When data capture is web-based, the calculations may be shuttled between the clinical site and data management office almost instantly. That rapid exchange optimizes every stage of trial conduct. Real-time scoring at screening visits can stratify participants into cohorts. Scores that signal an adverse event can immediately trigger workflows for stabilizing the participant and submitting safety reports. When the time comes to analyze results, a portion of the statistical labor is already done.
Can you give me an example?
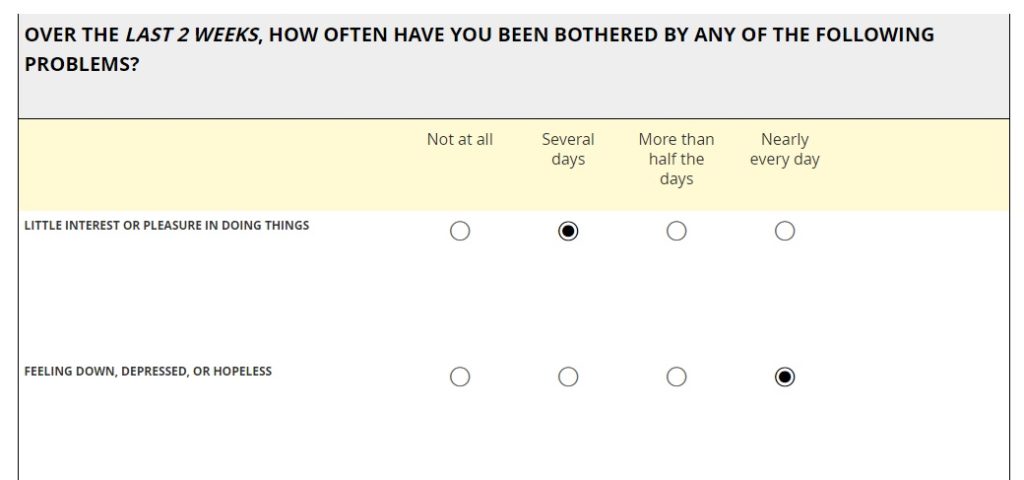
I was hoping you’d ask. Below you’ll find two presentations of the Patient Health Questionnaire-9 (PHQ-9), an instrument for screening, diagnosing, monitoring and measuring the severity of depression. The first presentation assumes out-of-clinic, ePRO use, where study managers expect most participants to respond on their own smartphone. The form will render on any web-enabled device, but the pagination is set to display one item at a time, for ease-of-use on smaller screens. The second presentation assumes in-clinic use on a tablet. Depending on the protocol, the researcher may administer the PHQ-9 through an interview with the participant, or the participant may complete the questionnaire on her own. In both cases, best practices in ePRO form design dictated layout and behavior.
OpenClinica forms support real-time scoring through syntax any data manager can learn quickly. Data managers have complete control over when and if the score is displayed on the form, rather than simply saved to the database. Scores may be built into forms for patient-reported outcomes (ePRO) as easily as they are for clinic visit forms. And conditional logic can trigger additional questions or other workflows based on specific scores.
So give your study’s major eClinical system a chance to do what it does best, and score one for speed and accuracy.